
Page 70 - Coespu 2020-2
P. 70
MEDICAL
mental state and 31% experienced are common in the acute stage ronavirus epidemics, but there
stroke, which were the most com- of SARS, MERS, and COVID-19; are few data yet on COVID-19.
mon neurological symptoms. Pa- •there is evidence of depression, In SARS and MERS in the acute sta-
tients also experienced headache anxiety, fatigue, and post-trau- ge, using data from two studies,
(12%), seizure (9%) and dizziness matic stress disorder in the the most important fi nding was that
(4%), among other symptoms. post-illness stage of previous co- confusion occurred in 27·9% of pa-
SARS-CoV-2 invades human host
cells by the angiotensin-converting
enzyme 2 receptor (ACE2r), which
has little expression in the brain.
There has been hypotesis that
other routes of CNS infi ltration
might account for the respiratory
failure caused by infection with
SARS-CoV-2, although there isn’t,
actually, evidence.There is prelimi-
nary in-vitro evidence that SARS-
CoV-2 can replicate in neuronal cel-
ls, but the translation of this fi nding
to in-vivo settings remains unclear.
Previous infl uenza pandemics
have been associated with long-la-
sting neuropsychiatric consequen-
ces, so it is possible that other viral
infections on a large scale could
cause sustained mental morbidity.
From a systematic review and me-
ta-analysis of the psychiatric con-
sequences of coronavirus infection
published by “The Lancet” in May
2020, were identifi ed 72 indepen-
dent studies that provided data
on both the acute and post-illness
psychiatric and neuropsychia-
tric features of coronavirus in-
fection, including seven medRxiv
preprints (Medrxiv is an Internet
site distributing unpublished ma-
nuscripts about health sciences).
The scientifi c literature predomi-
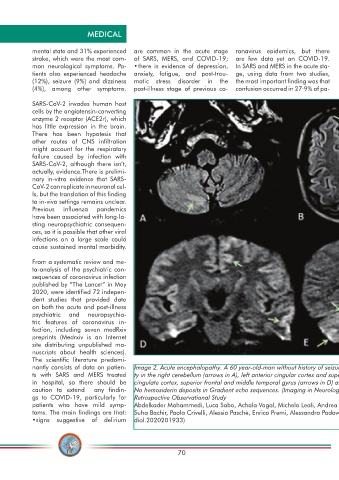
nantly consists of data on patien- Image 2. Acute encephalopathy. A 60 year-old-man without history of seizures presenting with convulsion. (A-B) Multifocal areas of FLAIR hyperintensi-
ts with SARS and MERS treated ty in the right cerebellum (arrows in A), left anterior cingular cortex and superior frontal gyrus (arrows in B). (C-D) Restricted diffusion in the left anterior
in hospital, so there should be cingulate cortex, superior frontal and middle temporal gyrus (arrows in D) and right cerebellum (arrows in E), consistent with cerebellar diaschisis. F)
caution to extend any fi ndin- No hemosiderin deposits in Gradient echo sequences. (Imaging in Neurological Disease of Hospitalized COVID-19 Patients: An Italian Multicenter
gs to COVID-19, particularly for Retrospective Observational Study
patients who have mild symp- Abdelkader Mahammedi, Luca Saba, Achala Vagal, Michela Leali, Andrea Rossi, Mary Gaskill, Soma Sengupta, Bin Zhang, Alessandro Carriero,
toms. The main fi ndings are that: Suha Bachir, Paola Crivelli, Alessio Paschè, Enrico Premi, Alessandro Padovani, and Roberto Gasparotti https://pubs.rsna.org/doi/10.1148/ra-
•signs suggestive of delirium diol.2020201933)
70